
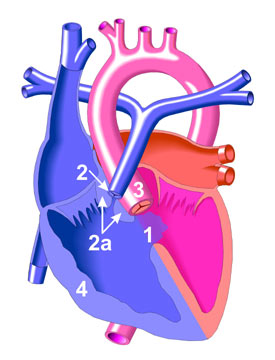
Tetralogy of Fallot occurs when there is a deviation of the development of the muscular septum of the ventricles antero-cephaladly. This would result in 3 of the 4 features of the 'tetralogy':
- Ventricular septal defect (VSD)
- Pulmonary stenosis
- Over-riding of the aorta
- Right ventricular hypertrophy (Secondary to compensation of the ventricles from pulmonary outflow obstruction)
These defects result in mixing of oxygenated and deoxygenated blood between the VSD from a left-to-right shunt outflow of mixed blood into the aorta causing cyanosis. Cyanosis is worsened when the pulmonary outflow tract is severely restricted and made worse during exacerbation hypercyanotic spell also known as Tet spell.
Compensation may occur via a patent ductus arteriosus (PDA) in newborns and major aortopulmonary collateral arteries (MAPCA).
Clinical Features:
- Cyanosis. In mild to moderate cases cyanosis may be absent depending on the severity of the pulmonary outflow obstruction.
- Hypercyanotic spells or Tet spell.
- Worsening early in the morning when crying or on exertion or vigorous activities.
- May be severe to result in unconsciousness.
- Hypoxia may occur to varying degrees which may progress the metabolic acidosis.
- Failure to thrive
- Delayed puberty
- Clubbing
- Parasternal heave
- Systolic thrill and ejection systolic murmur usually heard over the upper parasternal area due to pulmonay obstruction.
- Murmur maybe almost absent in hypercyanotic spells due to complete obstruction of the pulmonary outflow tract.
- Echocardiography: Standard modality for diagnosis. Able to outline extent of defects.
- Chest X-ray:
- Coeur en sabot: Boot shaped heart
- Right-sided aortic arch
- Diminished pulmonary vasculature (not prominent)
 | |
| Boot-shaped heart with right ventricular enlargment. |
- ECG:
- Right axis deviation
- Prominent R wave on right precordial chest leads and S wave in lateral precordial chest leads.
- Bifid P wave
- Polycythemia
- Cerebral thromboses in severe cases of polycythemia
- Infective endocarditis
- Brain abscess
References:
1. Kliegman, Robert M., et al., Nelson Textbook of Pediatrics, 18th ed., Elsevier Saunders.
2. Doyle, T., et al., Pathophysiology, Clinical Features and Diagnosis of Tetralogy of Fallot, UpToDate article, (2013).
3. Bailliard, F., et al, Tetralogy of Fallot.
Future Topics:
- Management of TOF
- Surgical Management of TOF
- Cyanotic heart disease
- Transposition of Great Arteries.
Nice and informative post. Please write about congenetal acyanotic heart diseases. Is there any treatment for patent ductus artariosus?
ReplyDelete